Rural Health Transformation Program: What the Criteria Suggest for Rural Healthcare in the Years Ahead

![]() by E. Cusaac for CHUG
by E. Cusaac for CHUG
CMS has begun implementing the Rural Health Transformation Program (RHTP), a multi-year funding initiative focused on rural healthcare systems. While the program has received attention for its scale, the more meaningful questions for healthcare organizations are structural: how the program is designed, how funding decisions flow, and what conditions states are expected to meet over time.
Why this matters:
The Rural Health Transformation Program is often discussed in terms of funding size, but its structure, guardrails, and performance requirements will shape how states and rural organizations actually experience it. This post breaks down how the program is designed, what the criteria emphasize, and where execution will matter most over time.
This post focuses on what the published criteria and guidance suggest about how RHTP is likely to operate in practice, and what that may mean for rural providers, administrators, technology partners, and community organizations.
How the Program Is Structured
RHTP is built around a state-led model. States apply to CMS, receive funding, and define how that funding is deployed through state-specific strategies, awards, and partnerships. Individual clinics and organizations do not apply directly to CMS, but instead participate through state-level pathways.
At the national level, CMS groups allowable initiatives into a small number of broad categories. These categories effectively define what states are incentivized to prioritize when designing their rural health transformation strategies.
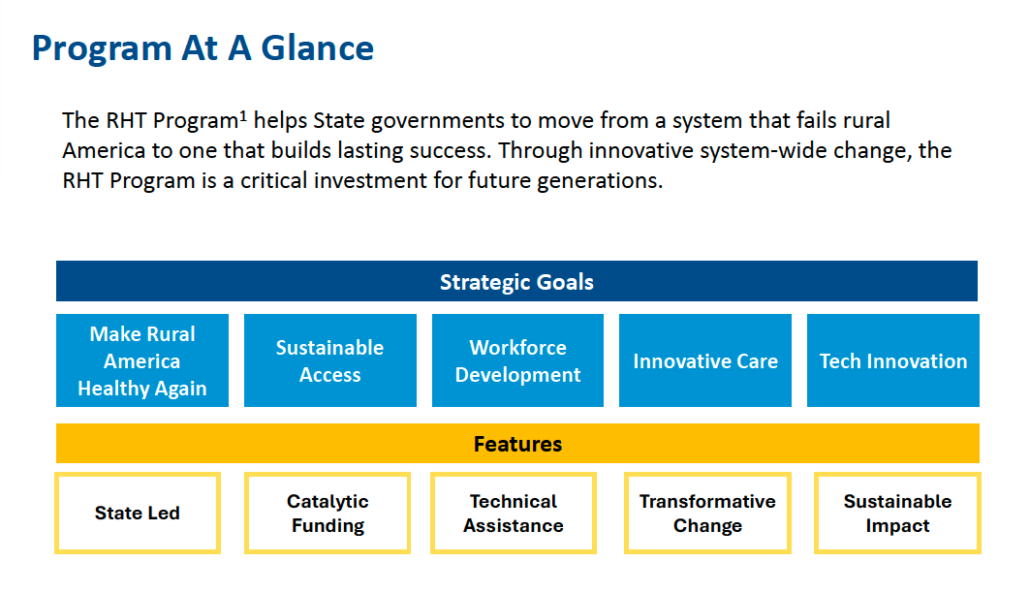
RHTP Strategic Goals: CMS groups rural health “transformation” into a small set of goal categories that shape how states design their programs.
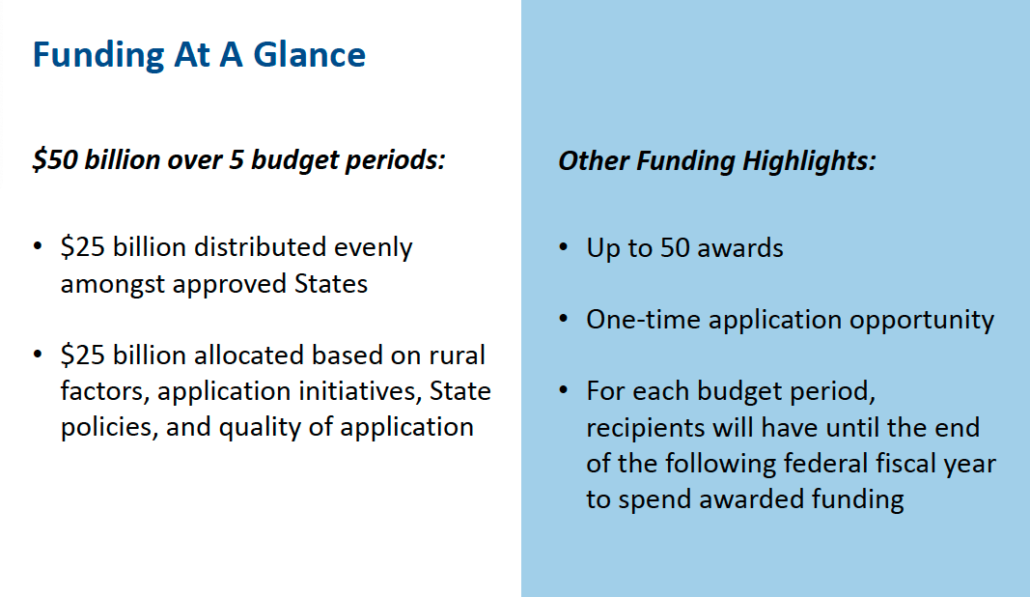
Funding at a glance: total program funding is distributed across multiple budget periods, with a mix of baseline and performance-linked components.
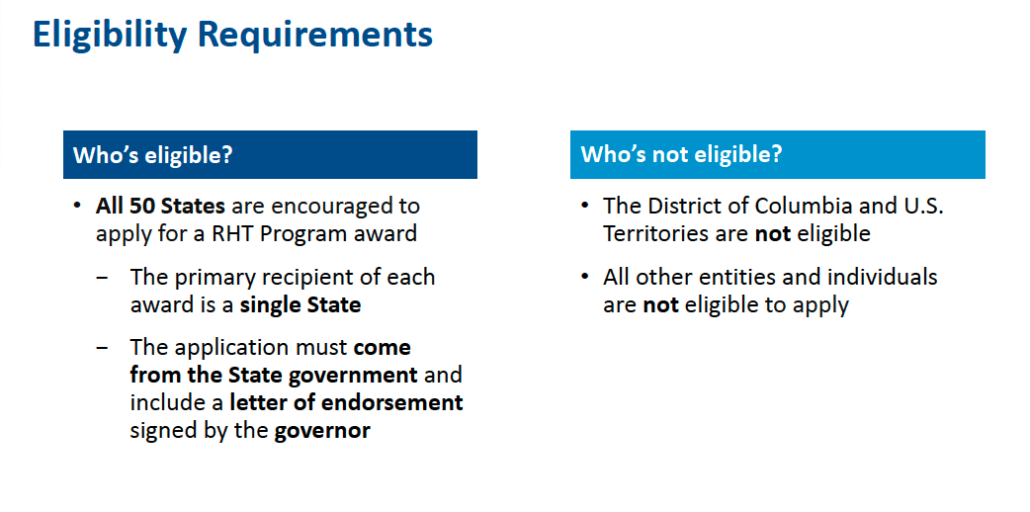
Eligibility requirements: RHTP is state-led, with states serving as the primary applicants and coordinators of funding.
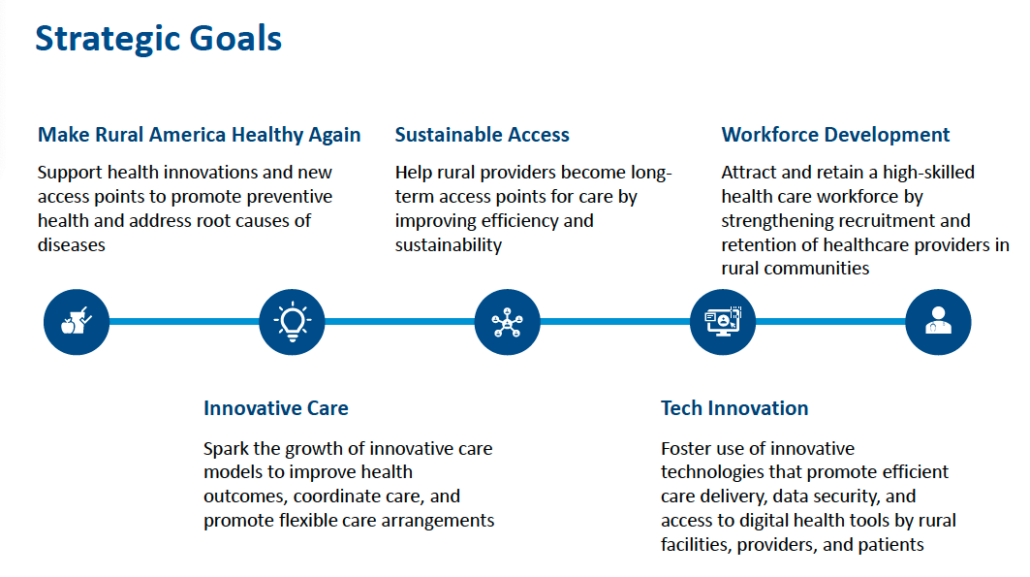
Strategic goal areas include access, workforce, care delivery innovation, and technology, which collectively frame what CMS considers “transformation.”
Rather than prescribing specific programs, CMS establishes these goal areas as guardrails. States retain flexibility in how they interpret and operationalize them, which means real-world impact will vary significantly by geography, governance structure, and existing capacity.
What the Criteria Emphasize
Across the Notice of Funding Opportunity and CMS applicant guidance, several consistent patterns emerge.
- State accountability is central. States must define rural populations, identify target communities, and report progress annually. Funding levels can be revisited based on performance.
- Funding favors system-level change. The program prioritizes structural capacity such as workforce pipelines, shared services, care redesign, and data infrastructure over isolated fixes.
- Measurement is expected. States must connect initiatives to measurable outcomes related to access, quality, workforce stability, and efficiency.
- Timing and readiness matter. Early funding favors projects that can launch quickly, while later funding emphasizes sustainability and coordination.
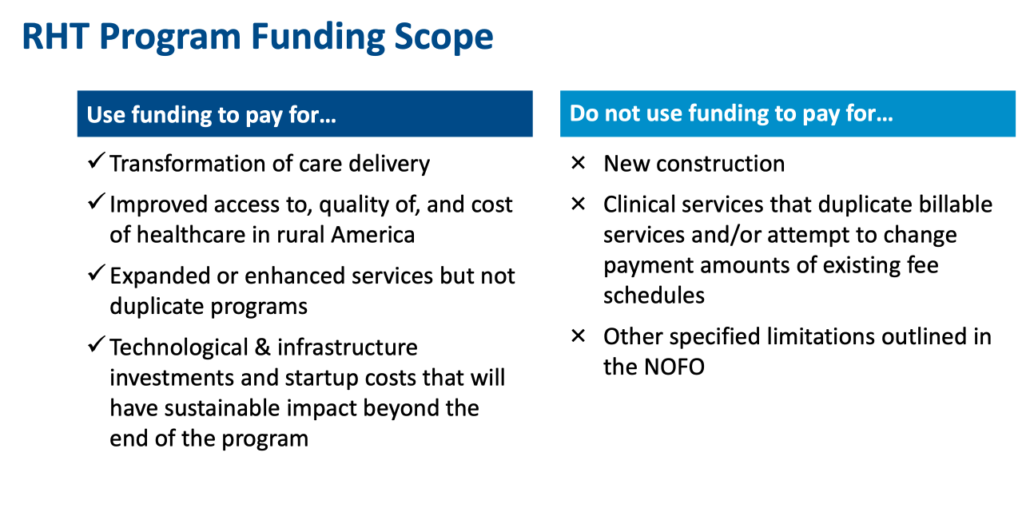
Funding scope: RHTP funds are intended for transformation and system improvement, not duplication of existing reimbursable services.
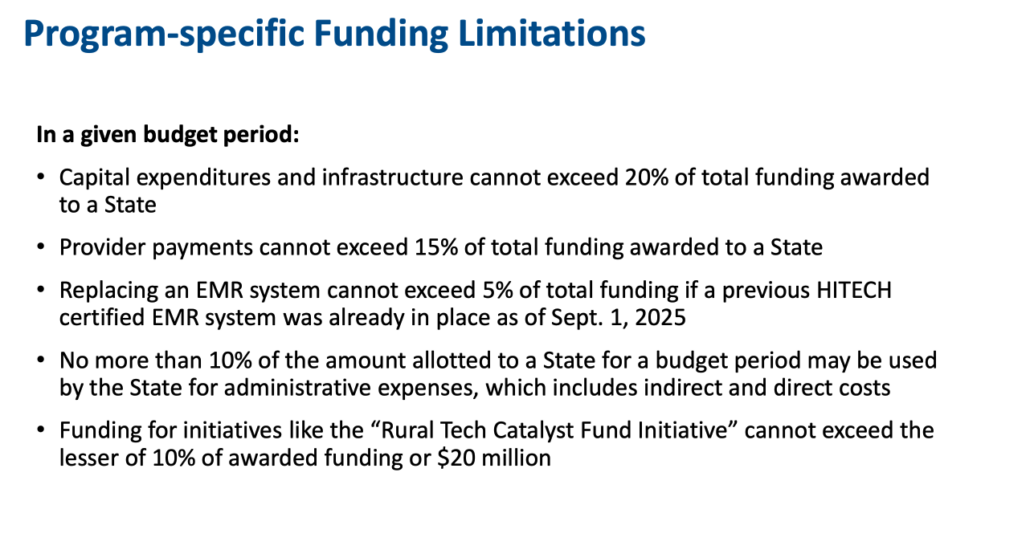
Funding limitations place caps on capital expenses, provider payments, administrative costs, and certain IT investments, shaping what initiatives can scale. These guardrails reinforce that RHTP is a targeted transformation program rather than general operating support.
How Funding Levels Are Determined Over Time
RHTP funding is not static. CMS separates funding into baseline amounts distributed to all approved states and workload-based funding that is recalculated over time.
Workload funding is tied to data-driven metrics, initiative progress, and state policy actions, meaning allocations can shift as states are reassessed.
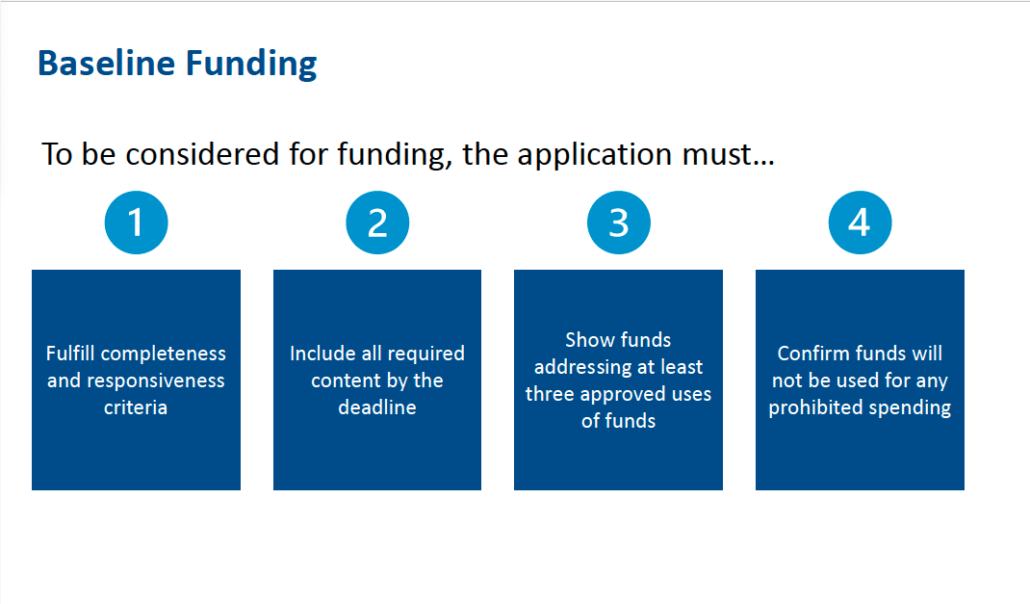
Baseline funding: states must meet minimum requirements to qualify for continued funding consideration.
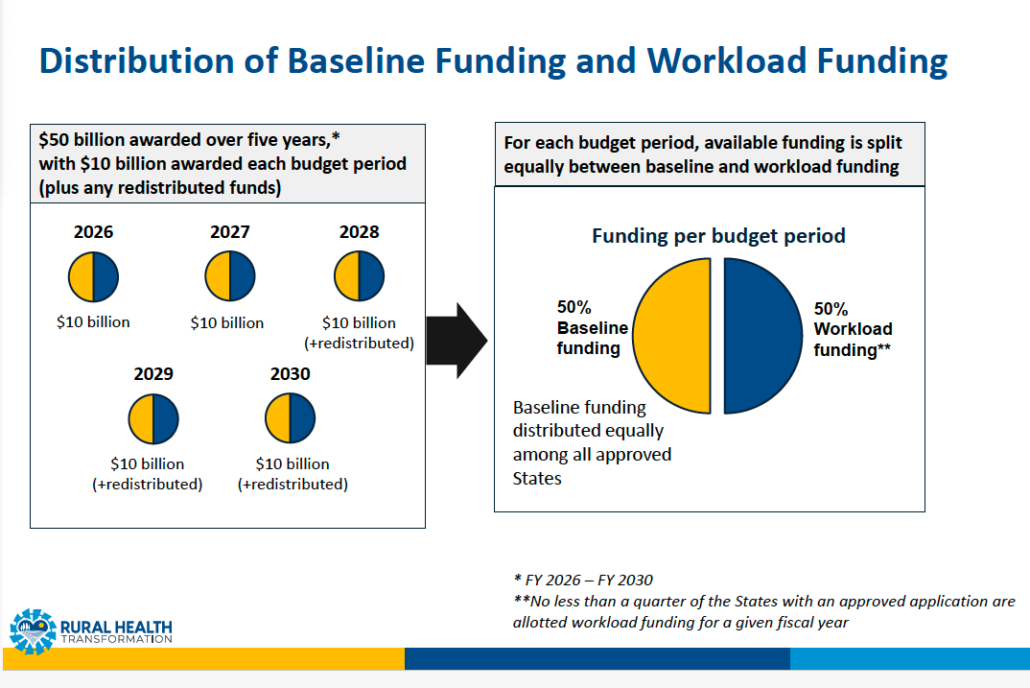
Funding distribution: available funds are split between baseline and workload components each budget period.
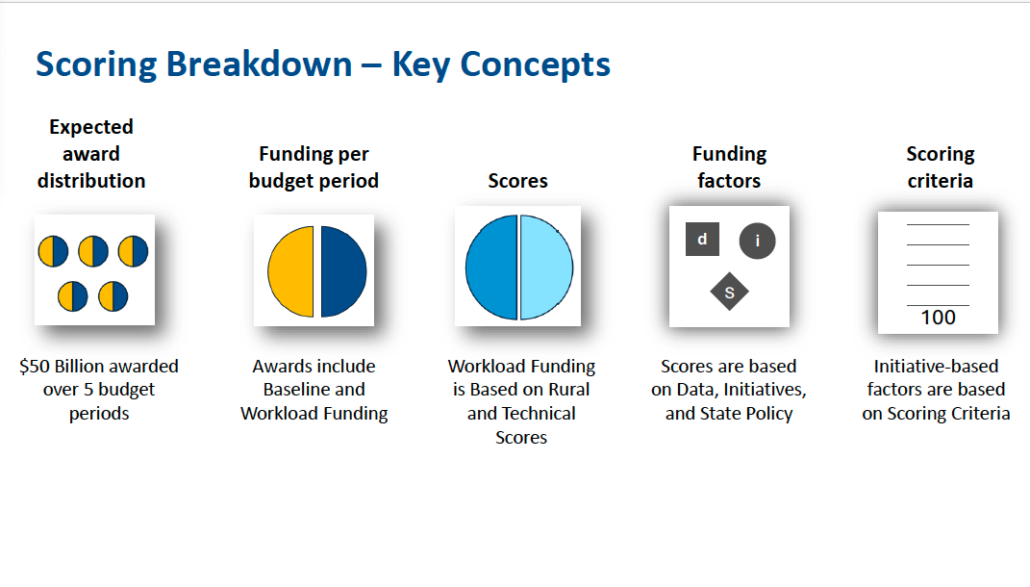
Scoring framework: workload funding is influenced by metrics, initiatives, and policy actions.
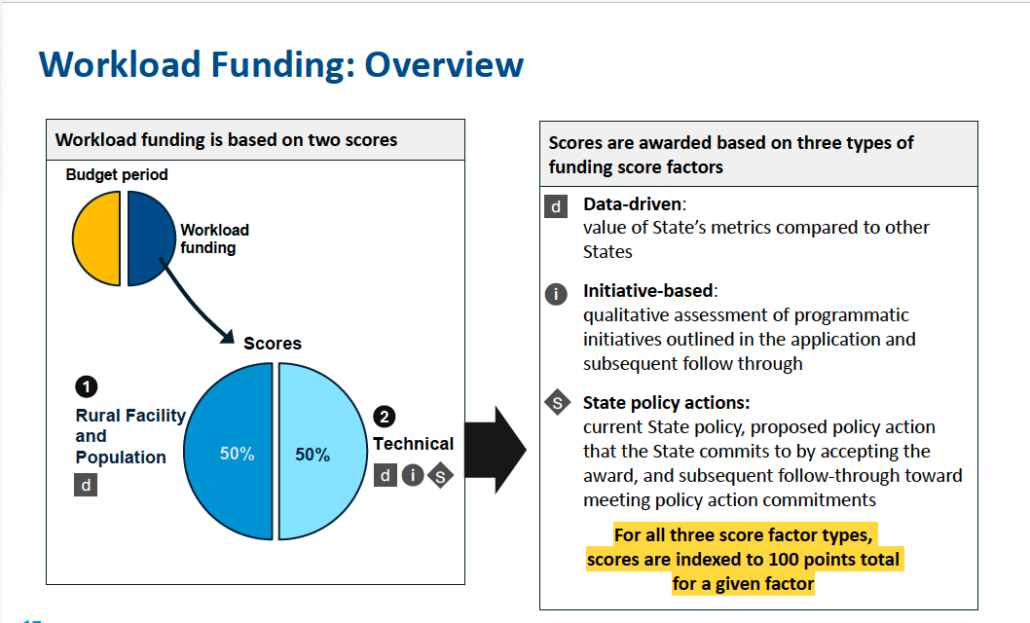
Workload funding overview: funding levels can increase or decrease based on execution and follow-through over time. For healthcare organizations, this structure means participation opportunities and funding availability may evolve based on state performance.
Why This May Matter for Rural Communities
Whether RHTP delivers meaningful benefit will depend largely on execution. That said, the program creates potential pathways to address challenges that are difficult to fund through traditional reimbursement models.
- How is your state translating national criteria into local priorities?
- Where does decision-making authority sit at the state level?
- What reporting and data requirements come with participation?
- Which initiatives are likely to be supported over multiple years?
Early Signals From State Implementation
While most states are still in early stages of planning, some have begun outlining how they intend to operationalize the Rural Health Transformation Program. These early signals are useful not as proof of outcomes, but as insight into how states may translate federal criteria into real programs.
Oregon, for example, has announced its initial RHTP award for 2026 and described a phased approach to deployment, including early funding for projects that can launch quickly followed by later rounds focused on readiness and sustainability.
This approach mirrors the flexibility CMS allows states, while also underscoring how much variation is likely across the country. Other states may take different paths based on governance structure, rural composition, and existing infrastructure.
What to Watch Going Forward
RHTP is best understood as a framework rather than a guarantee. Its impact will vary by state, by community, and by how closely funding priorities align with operational realities.
We will continue tracking how this program evolves and what it means for rural healthcare delivery, operations, and supporting technology.
As states move from application to implementation, more detailed plans are beginning to emerge. In a follow-up post, we’ll look at how one state (Oregon) is translating CMS criteria into timelines, funding pathways, and operational decisions, and what that may signal for rural organizations navigating similar processes elsewhere.
#chugusers #CHUGCHAT
Source Materials and Reference Links
- CMS Rural Health Transformation Program Overview
https://www.cms.gov/priorities/rural-health-transformation-rht-program/overview
- CMS RHTP Applicants Webinar Presentation (PDF)
https://www.cms.gov/files/document/rht-program-applicants-webinar-presentation.pdf
- RHTP Notice of Funding Opportunity (NOFO)
https://files.simpler.grants.gov/opportunities/782f996f-78f8-4742-8b68-d2bf50c87f99/attachments/1f9b7812-12a9-46ab-92cf-bb804c0bf6ac/cms-rht-26-001_final.pdf
- KFF: Key Takeaways From CMS’s Rural Health Funding Announcement
- National Rural Health Association – RHTP Summary
https://www.ruralhealth.us/programs/center-for-rural-health-innovation-and-system-redesign/rural-health-transformation-program

